2023-04-05
ATTRv patients, including Skelleftesjukan, receiving a ‘single shot’ towards a cure
The 23rd of November, 2021 the first patient in Sweden was treated with a CRISPR-Cas medicine aimed at permanently modifying a diseased gene towards a cure for hereditary transthyretin amyloidosis (ATTRv). The administration was part of a world first in human genetic modification clinical trial sponsored by Intellia Therapeutics, the company co-founded in 2014 by Jennifer Doudna, who in 2020 along with colleague Emmanuelle Charpentier won the Nobel Prize in Chemistry for development of the CRISPR-Cas9 genome editing technique.
Emmanuelle Charpentier was employed at Umeå University 2008 till 2013 where she published some of the work leading to her nobel prize. This marked the beginning of a decades long interaction in development of this medicine for Swedish ATTRv patients. Roughly 240 of Sweden’s 400 ATTRv patients live in the north of Sweden, specifically in the Norrbotten and Västerbotten regions, the latter of which Umeå is the capital. The majority of Swedish patients suffer ATTRv caused by the prevalent V30M mutation (Skelleftesjukan), but there are 15 other mutations in Sweden that may be treated by NTLA-2001.

Björn Pilebro
The investigational medicine NTLA-2001 is intended to be a ‘one time’ treatment for patients would otherwise normally die within 4-17 years after the onset of symptoms. This ground breaking clinical trial is being held at 4 sites around the world; Paris/France, Auckland/New Zealand, London/UK and Norrlands universitetssjukhus in Umeå/Sweden. Umeå based clinician Björn Pilebro has been treating patients with ATTRv for over ten years now and is responsible for the Swedish site of the trial. “To date we have treated nine Swedish patients in the study and we have not seen any severe side effects. With patient follow up at one year we see a durable and potent reduction in transthyretin after one infusion of the CRISPR/Cas-9 based pharmaceutical”, says Björn.
ATTRv has a diversity of effects on patients including peripheral nerve, heart, digestive, eyes and kidney problems. The disease was first described in medical literature by the German neuropathologist Friedrich Wohlwill 1942. Symptoms often begin in adults as numbness in feet, lower legs and sometimes hands. Weakness in arms and leg muscles follows, weightloss due to digestive issues and heart arrythmia. With time organ failure including heart and kidney. As transthyretin, the disease causing protein, is produced in the liver, liver transplantation was the only treatment 10 years ago.
Björn tells of developments in the last decade. “Liver transplantation can be seen as a crude, but in many patients very effective, ‘gene therapy’, eliminating the production of faulty transthyretin and halting disease progression. We were pleased to see several medicines in the last decade targeting transthyretin RNA and reducing circulating protein in the absence of unwanted effects of the protein loss. We are continuing to follow the patients in the study for 18 years after treatment.”
The first-ever clinical data for in vivo CRISPR genome editing was published in the New England Journal of Medicine in August 2021 (Gillmore et. al. 2021), demonstrating Phase I safety in 6 patients. This was followed up in June 2022 with data showing NTLA-2001 showed durable reduction in disease-causing protein out to at least 12 months, following a single-dose treatment. The estimated completion data for the study is March 2026.

Örjan Norberg
Örjan Norberg works to drive patient access to life saving medicines in Västerbotten region and has been a central figure in the National projects CAMP and Swelife-ATMP, in particular the health economy project. “It is a fantastic break through if we can cure patients that have severe chronic diseases. One challenge though with these new medicines is that they often come with a very high price tag, which is a great budget challenge for healthcare, and will become an even greater challenge in the future when more of these types of treatment are approved.”
Indeed, there are three medicines approved for treatment of ATTRv; tafamidis, inotersen and patisiran. Tafamidis acts on transthyretin in the blood stream, stabilizing it in its functional form and thus reducing the rate of amyloid formation. The oligonucleotide-based medicines inotersen and patisiran have been shown to effectively reduce disease causing protein in many patients by RNA in patient liver cells, though long-term treatment results in, for patisiran, continued exposure to premedication glucocorticoids and antihistamines and for inotersen, risk of haematological side effects. These medicines need to be administered in a clinic every third week and for life, as no permanent genetic modification is made. A curative CRISPR/Cas9 solution may require payment upfront, for life, a model healthcare systems are not prepared for.
“Providing patients with medicines that not only markedly reduce their disease symptoms but suit them living as normal life as possible, and are affordable to the public health system, is the ultimate success”, says Björn.
More information:
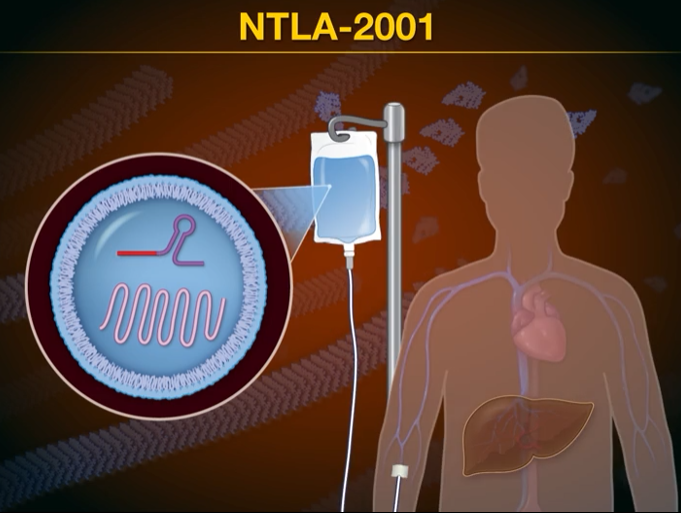
The investigational medicine NTLA-2001 contains messenger RNA for Cas9 protein and a single CRISPR guide RNA targeting TTR encased within a proprietary lipid nanoparticle (LNP). The proprietary LNP is essential for precisely delivering CRISPR/Cas9 to the liver, following IV infusion over several hours, where it inactivates TTR on chromosome 18 in hepatocytes by causing a permanent frameshift mutation, reducing disease causing protein. NTLA-2001 inactivates both ‘wildtype’ and hereditary diseased TTR, thus being used in this clinical trial for treatment of both Transthyretin Amyloidosis-Related Cardiomyopathy (ATTR-CM), normally developing in the elderly without gene mutation, and Hereditary Transthyretin Amyloidosis With Polyneuropathy (ATTRv-PN), ATTRv developing in younger individuals with the TTR mutation. The functions of transthyretin in transporting vitamin A and thyroid hormone are also performed by other substances in the blood, so loss of the protein is not expected to and has not shown to have severe consequences. The proprietary targetting to the liver intends that the gene modification does not occur in other cell types of the body, thus cannot be passed to future children.
LINKS:
http://www.umu.se/nyheter/skelleftesjukan-forst-ut-att-behandlas-med-gensaxen-_11647272/
http://lakartidningen.se/aktuellt/nyheter/2022/11/gensaxen-behandlar-skelleftesjuka/